
Tear trough filler exists because faces age in inconvenient ways. Bone resorbs, fat shifts, skin thins, and suddenly your under-eyes look like they've been pulling all-nighters without your permission. When used properly, a small amount of hyaluronic acid filler can soften the hollow between the lower eyelid and the cheek, reducing shadowing and making you look more rested — not "done."
But here's the part Instagram conveniently crops out: it doesn't fix eye bags, tighten loose skin, or magically erase pigmentation. And if the anatomy isn't right, filler won't save the day — it'll make it worse. That's why tear troughs are less about injecting and more about knowing when not to. The best tear trough consultations end with "no." Most patients don't want to hear that. The good ones are grateful for it later.

Why Under-Eyes Hollow in the First Place
The tear trough isn't a wound, a defect, or something that went wrong. It's anatomy doing what anatomy does — changing over time. What people call "dark circles" is usually one of three things, or a combination of all of them:
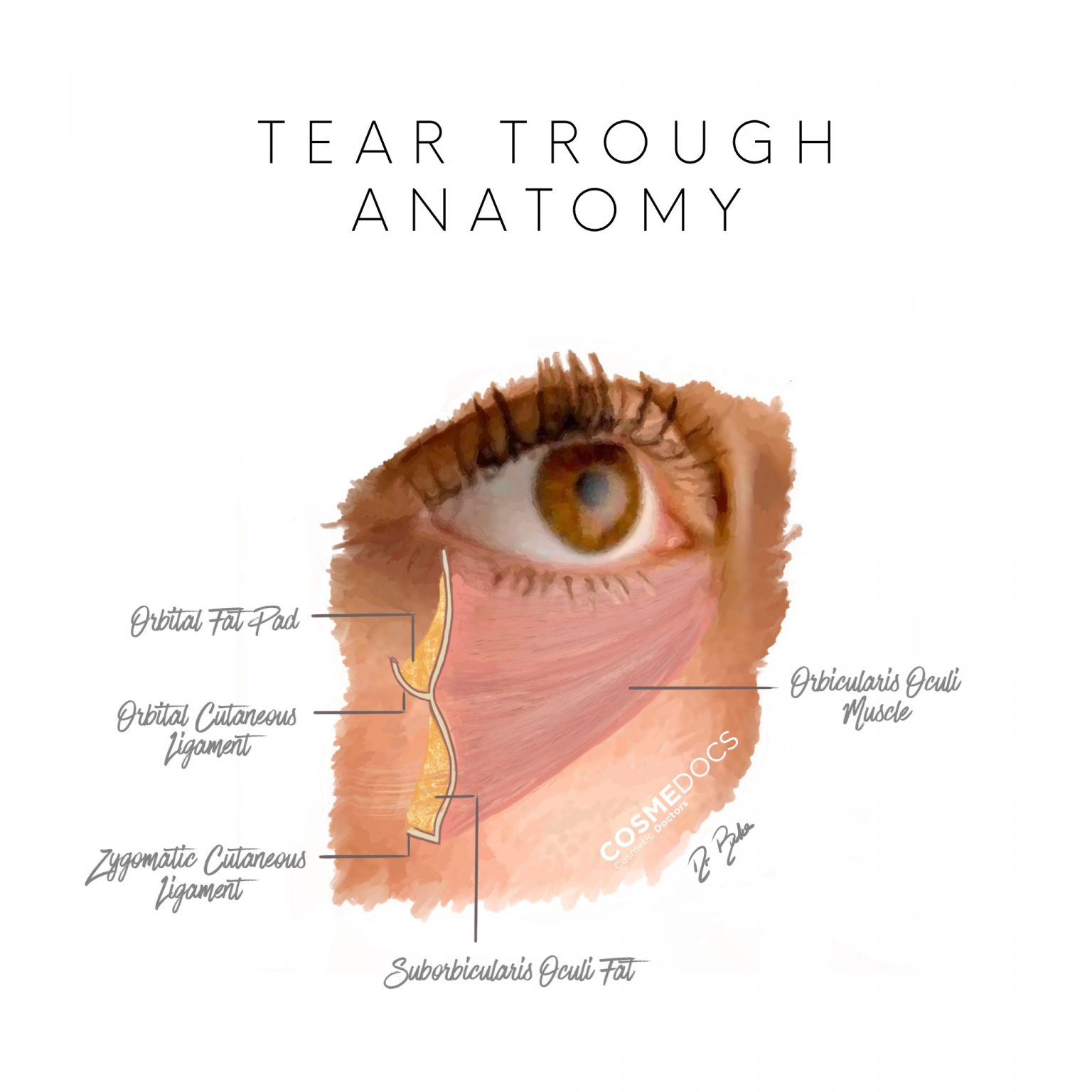
- 01Volume loss. The fat pads beneath your eyes sit on a bony shelf. As bone resorbs and fat descends, a groove appears. Light falls into it. Shadow forms. You look tired even when you're not.
- 02Skin thinning. The skin beneath the eye is the thinnest on the body — roughly 0.5mm. As collagen depletes with age, the underlying orbicularis oculi muscle and blood vessels become more visible. This creates a bluish-purple hue that no concealer quite fixes.
- 03Genetic predisposition. Some people are born with a deeper tear trough. They've looked tired since their twenties. Their mum probably has the same thing. Ageing just makes the contour more pronounced.
Why Tear Trough Fillers Sometimes Fail
Let's be direct about something most clinics don't volunteer: tear trough filler is one of the treatments most likely to go wrong in the wrong hands. The margin for error is smaller here than almost anywhere else on the face. Here's why:
Wrong candidate, right filler
If the cause of dark circles is pigmentation, not volume loss, adding filler won't help. It may even make things worse by creating a fullness that catches light differently. The darkness remains, but now there's a bump under it.
Too much product
The under-eye area tolerates very small volumes — typically 0.3 to 0.5ml per side. More than that and the skin begins to look puffy or swollen. The irony is that over-filled tear troughs often look more tired than the untreated version.
Wrong product
Not all hyaluronic acid fillers are created equal. The under-eye requires a soft, low-cohesivity product that integrates smoothly beneath tissue-paper-thin skin. Using a product designed for cheeks or jawlines in the tear trough is like using a sledgehammer to hang a picture frame. It'll stay up. It won't look right.
Tyndall effect
If filler is placed too superficially beneath thin skin, it can scatter light and create a bluish discolouration — the Tyndall effect. It's not dangerous, but it's visible, and it doesn't resolve on its own. It requires dissolving.

Interpreting Tear Trough Results: What Improvement Looks Like
Good tear trough results are the ones you barely notice. The goal isn't to eliminate every shadow or erase every line — it's to soften the hollow just enough that people stop asking if you're tired, and start asking if you've been on holiday.

In the image above, filler has been placed deep, with precision, using a product designed specifically for the periorbital area. The improvement is visible but not dramatic — which is exactly the point. The patient looks rested, not altered. That's what restraint looks like when it's done by someone who understands the anatomy.

Notice how the contour of the lower eyelid transitions more smoothly into the cheek. There's no puffiness, no ridge, no visible product. The filler has been placed in the correct plane, at the correct volume, in the correct patient. Three things that all need to be right simultaneously.
Who Should Not Have Tear Trough Filler
This might be the most useful section on the entire page. Because the truth is, a significant number of people who want tear trough filler shouldn't have it. Not because there's anything wrong with wanting it — but because filler won't give them what they're looking for.
You may not be suitable if:
- —Your dark circles are primarily caused by pigmentation (melanin deposit), not shadowing from volume loss
- —You have significant lower eyelid fat prolapse (eye bags) that would need surgical correction
- —Your skin is very thin and crepey, with poor elasticity — filler placed here may become visible or create irregularities
- —You're prone to significant swelling (malar oedema) in the mid-face area
- —You've had multiple previous filler treatments in the area without dissolution — residual product can accumulate unpredictably
A good consultation doesn't just assess what filler can do — it identifies what filler can't do, and tells you honestly.
Why Injector Skill Matters More Here Than Almost Anywhere
Most cosmetic treatments have a reasonable margin of error. Lip filler can be dissolved. Botox wears off. But tear trough filler sits in a uniquely unforgiving area — thin skin, complex vascular anatomy, and a structure that changes with every facial expression. There is almost no room for approximation.
The difference between a smooth, natural result and a visible, lumpy one often comes down to millimetres of depth, fractions of a millilitre of product, and — most critically — the decision about whether to treat at all. The best injectors aren't the ones who say yes most often. They're the ones who say no when the anatomy doesn't support it.
"In tear trough treatment, the most important skill isn't injection technique. It's patient selection."
— Dr Ahmed Haq, Medical Director, CosmeDocs
When Filler Isn't the Answer: Polynucleotides for Tear Troughs
For patients whose under-eye concerns are more about skin quality than volume loss — fine lines, crepiness, a dull or dehydrated appearance — polynucleotide therapy offers an alternative approach. Rather than adding volume, polynucleotides stimulate tissue regeneration at a cellular level, improving skin texture, hydration, and elasticity over a course of treatments.

Polynucleotides aren't a replacement for filler — they do different things. But for patients who aren't candidates for tear trough filler, or who want to complement filler with improved skin quality, they represent a genuinely useful option. The improvement is gradual rather than immediate, and typically requires two to three sessions.
Frequently Asked Questions
Can tear trough filler fix dark circles?
It depends entirely on the cause. If your dark circles are shadows created by volume loss, filler can make a visible difference. If the darkness is pigmentation — melanin deposited in the skin — filler won't change that. A proper assessment determines which is which before any treatment is considered.
Why do some tear trough results look unnatural?
Usually because of overcorrection, wrong product choice, or treating patients whose anatomy wasn't suited to filler. The under-eye has very thin skin and limited space — even small misjudgements become visible. This is why the area demands more experience, not less.
What's the difference between tear trough filler and polynucleotides?
Filler physically restores volume to the hollow. Polynucleotides stimulate tissue regeneration and improve skin quality without adding volume. They serve different purposes and can be complementary, but they're not interchangeable.
How do I know if I'm suitable?
An in-person consultation. Photographs and online assessments can suggest suitability, but the under-eye area requires direct assessment of skin thickness, fat distribution, and the relationship between the orbit and cheek. There's no shortcut for this.
Visual Evidence
For a comprehensive collection of clinical photographs, visit our tear trough filler before and after results.
The most useful results aren't the most dramatic ones. They're the ones where the patient looks rested, not altered. That's the invisible art. That's what good treatment is supposed to do — improve without announcing.
Results vary depending on individual anatomy, skin quality, and degree of volume loss. A consultation is required to assess suitability.
Treatment Page
Tear Trough Filler Treatment
If you're considering treatment and want to understand what's involved, suitability criteria, and expected outcomes, the treatment page covers it in detail.
Learn about tear trough filler treatment →About the Author
Dr Ahmed Haq is the Medical Director of CosmeDocs, practising from 10 Harley Street since 2007. He specialises in structural facial contouring, non-surgical rhinoplasty, and training physicians at the Harley Street Institute. His approach prioritises anatomical assessment over aesthetic trends — treating what the face needs, not what social media suggests.
Dr Haq's conservative approach to tear trough treatment reflects over a decade of managing patient expectations in this high-sensitivity area. This article addresses the clinical realities he discusses in every tear trough consultation — including when filler is not the answer.
Experience
17+ years in aesthetic medicine · 1M+ procedures since 2007
Memberships
- ·Royal College of Physicians (RCP)
- ·British Association of Cosmetic Doctors (BACD)
- ·Harley Street Institute — Faculty Trainer
Clinical Specialities